
Entries by Scott McPherson (423)
Death returns to Riau
 Scott McPherson
in influenza and infectious diseases
|
Scott McPherson
in influenza and infectious diseases
|
 Post a Comment
Post a Comment
 Authorities are returning to Riau, Indonesia, in the wake of another suspected family cluster (for reference, see my earlier post All Eyes on Riau, http://www.scottmcpherson.net/journal/2007/10/8/all-eyes-upon-riau-indonesia.html ).
Authorities are returning to Riau, Indonesia, in the wake of another suspected family cluster (for reference, see my earlier post All Eyes on Riau, http://www.scottmcpherson.net/journal/2007/10/8/all-eyes-upon-riau-indonesia.html ).
Over the weekend, 10 year old Gozi Sultia Ningsih died of a confirmed H5N1 infection. Her 17-year old aunt, Riri Rianti, also died after being hospitalized on October 11, but, incredibly, no samples were taken for analysis. Just how, in perhaps the most bird flu-ridden province in Indonesia, can no samples be taken of a young girl with suspected H5N1 symptoms?! This is beyond the imagination of any competent medical professional or layperson.
This fact is not lost on the central government in Jakarta, which is growing increasingly frustrated with the inability of local medical authorities to observe suspected human H5N1 protocols. The exasperation is clearly noticeable in the quotes from Dr. H Djuharman Arifinof, chairman of the Dewan Perwakilan Rakyat Daerah (DPRD), or Regional Council of Representatives, representing the Riau district.
The following is again from intrepid Flu Wiki/Flutrackers poster and nimble-fingered lay translator Commonground. Don't try to read each word literally; scan the translation and then read between the lines.
Related To Fall Again Casualties Flu Burung
All Element Must Work Extra
22 Oct 2007 14:32 wib
Pekanbaru (RiauInfo) - Rep. Chairman DPRD Riau, Drs H Djuharman Arifin, APT, MP
require/demand/beg and summon to Government Province Riau Government Kota, Regency and all element must be able to carry out work extra towards handle matter of suspect flu bird in Riau. Do not to the point of to wait for casualties new now this be handled.
"Yes, I feel method like that not effective which as long as this now we see someone manner handling when there is casualties to fall. Recent activity directly to fall toward location incident. Better Pemerintah Provinsi Riau should have step that accurate," say Djuharman Arifin toward RiauInfo in Kantor DPRD Riau, Senin (22/10). (bold mine)
According to Djuharman, matter that all important carried out toward prevention should have concept that clearly conveyed toward Government Center. Concept important which should be executed Pemerintah Provinsi Riau that is by give immunizatio to community in order thatthe immune to virus H5N1 mentioned. Second, question/issue/problem pountry should looked into/verified correctly in order that domestic animal poultry did not spread virus and third, Pemerintah Provinsi must be able make map/chart geographic region that endemic flu bird.
Until concept aforementioned be obtained exceed all problems which take place when this. Map region endemic that very necessary because we will be able to see someone who which infected/spread or which not infected/spread," he said.
For the moment that, Chief Commission D DPRD Riau, Ir Fendri Jaswir to augment before/not yet many to fall casualties soul Dinas Health Diskes and Dinas Peternakan must proactive task with the result that be able to overcome virus extinguish now (flu burung). The problem is from sum suspect flu bird more lacking/insuffient 23 people, 4 died, and 4 positive. (bold again mine)
http://www.riauinfo.com/main/news.php?c=6&id=2777
"Yes, it was positive (of bird flu)," she told reporters at the State Palace here.
The girl's aunt had died earlier of suspected bird flu, she added.
"But we are not certain about her aunt because we didn't take her blood sample," the minister said.
Talking Points: Top Ten reasons why we haven't had an influenza pandemic since 1968, and Top Ten reasons why we will have one, and probably soon (from July 2007).
Scott McPherson
in influenza and infectious diseases
|
Post a Comment
Admittedly, this is a rerun of a July, 2007 blog I wrote. But things are pretty slow right now on the avian flu front, and we need talking points to keep people focused on the Big Picture. So I felt a rehash of this old blog would be appropriate.
Scott 
With apologies to David Letterman, here is a quick list that you can keep handy and use to win arguments on the likelihood of an influenza pandemic. Feel free to add to this list, but it is written to be easily and quickly understood.
Top 10 reasons why we have not seen a pandemic since 1968:
10. The H5N1 virus has not “made it” around the globe – at least we have not seen high-path H5N1 yet in North America (at least none that any authority is willing to admit).
9. Surveillance of poultry and wildfowl, including aquatic wildfowl, has improved exponentially since 1968.
8. Rapid typing of influenza genetics allows public health officials to quickly make good decisions and move decisively to contain virus.
7. Education campaigns help to better promote awareness, especially in nations where H5N1 is becoming endemic. So when people get sick, or poultry gets sick, people are now a little more likely to report it.
6. Mass culling of poultry has beaten back the virus many, many times around the world. One major influenza researcher even went so far as to state that a pandemic strain of H5N1 has probably already died with a mass cull somewhere in this world.
5. Financial compensation for culled poultry helps convince some farmers to report deaths of poultry to the authorities.
4. The neuraminidase inhibitor antivirals (Tamiflu in particular) have been repeatedly effective in reducing H5N1 symptoms and ultimately in saving patients, but only in cases where a) the virus may not be as lethal, and b) when administered within 24 – 48 hours after onset of symptoms.
3. The WHO and global health authorities are ready to fly in supplies and “stamp out” outbreaks quickly. The August, 2006 “Tamiflu blanket” of 2,000 Indonesian villagers in four separate hamlets serves as evidence of the ability of public health authorities to combine Reasons #9, #8 and #5 into a coordinated action plan.
2. The Hong Kong government’s 1997 action to cull every bird in the city as the first suspected human-to-human transmission of the “new” H5N1 virus probably saved the world from a pandemic. Saved, or at least delayed the pandemic.
1. Global seasonal flu vaccine programs -- and the WHO's trying to pick the "Super Bowl winner" of three viruses (two Influenza A's and one B for the trivalent formula) in the February before the upcoming flu season -- have proven pretty accurate. They miss the B formulation more often than they miss the A, but still it has helped reduce the amount of seasonal flu, which helps reduce the potential for a pandemic. After all, each of us is a potential "mixing vessel" for a reassortant pandemic strain..
co-#1: We are damned lucky.
Top 10 Reasons why, despite all these efforts, we will still have a pandemic one day and probably soon.
10. H5N1 is becoming endemic in many parts of the planet, especially where people live in close physical proximity to poultry. It is a mutating fool and cleverly defies attempts to kill it. It is a supremely adept player at "King of the Mountain," which is the game all influenza viruses play.
9. Financial compensation for culled poultry helps somewhat, but the amounts paid usually are far short of actual losses incurred. If farmers do not feel that reporting avian flu losses are worth it in financial terms, they may (and already do) decide not to report the infections – unless their own family members become infected.
8. Smuggling of poultry, exotic birds and fighting cocks continues to accelerate. While not likely to be a principal source of spread of the disease, smuggling can nonetheless cause new outbreaks (ask the Vietnamese about their own “Ho Chi Minh Trail” issues along their border with China).
7. Modern industrial farming practices may actually and inadvertently encourage the spread of virus. Even a tiny particle of virus, trampled underfoot and brought into a poultry shed by a worker or farm machine, can kill thousands of poultry. And if left unchecked, even a “low path” avian flu can incubate, recombine with itself and emerge as a lethal, highly pathogenic influenza virus.
6. Despite the best 21st Century medicine and technology, avian flu of all types continues to spread and the frequency continues to accelerate. Witness the recent outbreaks of H7N2 in the Delmarva (Delaware, Virginia and Maryland) peninsula of the United States (2004), the H5N2 outbreak in West Virginia (2007), the outbreak of H7N7 in the Netherlands and other parts of Europe which killed a veterinarian and infected at least 89 people via human-to-human transmission and possibly hundreds more (2003), and the outbreak of H7N2 in Wales which also infected 17 humans (2007).
5. Globalization has also inadvertently encouraged the spread of virus. Witness the Bernard Matthews disaster of early 2007. Hungarian-raised poultry, shipped to England for processing, carried high-path H5N1 with it. This was introduced into one shed, and then workers carried the virus to three adjacent sheds. In the end, over 160,000 turkeys had to be killed and disposed of. The Hungarian poultry were contaminated, in all likelihood, by wildfowl droppings laden with H5N1 virus that were carried into turkey sheds.
4. Migratory wildfowl continue to transport the H5N1 virus, along with every other flu virus known to Humankind, in their bellies. Migratory wildfowl are the custodians and reservoir of avian influenza. As they shed virus, it either dies or is picked up by other creatures.
3. H5N1 has jumped the species barrier. In Indonesia, a study postulated that up to 20% of all stray cats in the archipelago nation showed antibodies to high-path H5N1. That means cats can be asymptomatic carriers of the most potentially lethal virus ever seen. The Indonesian television videos of Army regulars accompanying healthcare workers into residential neighborhoods to swab the mouths of housecats is chilling.
2. The only continents where H5N1 does not have a strong foothold are the Americas, Australia and Antarctica. H5N1 can be found from sub-Saharan Africa to the Middle East, most of Europe, Asia, and Indonesia. Only in Europe has human death not yet occurred from H5N1. Unfortunately, that statistic can be wiped out with a single transcontinental or transoceanic airplane flight.
1. History is against us. In the past 300 years, no fewer than ten influenza pandemics have ravaged the world. Some, such as 1918’s Spanish Flu and the pandemic from 1562–1568 were extremely lethal. The 1562 pandemic may have had a death rate higher than 1918’s, which is almost unthinkable. Others, such as 1889’s, had a less lethal but still severe effect on the planet.
The Devil you know
Scott McPherson
in Politics and government, Popular Culture, influenza and infectious diseases
|
1 Comment
|
 4 References
4 References
Sports teams, schools, hospitals wrestle with global MRSA epidemic
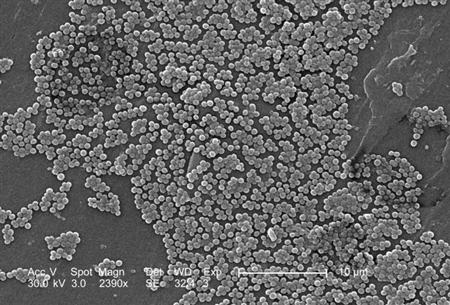 MRSA has claimed yet another young life. Seventeen year-old Ashton Bonds of Lynch Station, Virginia, died following a bout with the disease. MRSA is the acronym for Methicillin-resistant Staphylococcus aureus, a particularly nasty bacteria that is showing up all over the nation. In Mr. Bonds' case, MRSA had spread via his bloodstream, attacking his kidneys, liver, lungs and heart muscle.
MRSA has claimed yet another young life. Seventeen year-old Ashton Bonds of Lynch Station, Virginia, died following a bout with the disease. MRSA is the acronym for Methicillin-resistant Staphylococcus aureus, a particularly nasty bacteria that is showing up all over the nation. In Mr. Bonds' case, MRSA had spread via his bloodstream, attacking his kidneys, liver, lungs and heart muscle.
MRSA apparently began its life in hospitals. The probable cause grew from lax oversight of hospital infectious disease control protocols.
From a Bloomberg news story of December 19, 2005: http://www.bloomberg.com/apps/news?pid=10000103&sid=aQGnyaFWj2FA&refer=us :
Researchers are concerned especially about antibiotic resistant bacterial infections that arise in hospitals and spread to homes and crowded workplaces. The microbe, called methicillin-resistant staphylococcus aureus, or MRSA, is creating a health hazard in the U.S. dwarfing the threat posed by the H5N1 avian flu, said Steve Projan, vice president of protein technologies for Wyeth, the drugmaker that markets the Tygacil antibiotic.
``This is a hyper-virulent virulent bug,'' Projan said in a press conference at the Interscience Conference on Antimicrobial Therapy and Antibiotics on Friday. ``While we're very concerned about H5N1, we do have in front of us today this outbreak of community-acquired MRSA.'' (bold mine)
Increasingly, researchers are finding these drug-resistant infections outside the hospital, leading to concerns about widespread outbreaks of hard-to-treat microbes.
In some hospitals in San Francisco and Los Angeles, the new toxic strain is the leading cause of drug-resistant staph infections. More than half the MRSA's at the Harbor-UCLA Medical Center are the community-acquired strain, according to a study presented Dec. 17 by Cynthia Maree, an infectious disease specialist at the University of California, Los Angeles Geffen School of Medicine.
``That's more than twice the rate we had in 1999,'' she said in an interview at the conference. ``When patients make repeat trips to the hospital with the same strain, health workers will sometimes clean the patient's home,'' in an attempt to get rid of the source of infection, she said.
MRSA has become a major pain in the rear for school districts. It has hit sports teams especially hard -- especially those sports with a great deal of abrasion on hard surfaces, where the bacteria can transfer from skin to skin. As a result, athletic coaches and trainers are learning about MRSA in clinics and lectures at coaches conventions. Today, for example, wrestling coaches in several states are required to disinfect all wrestling mats after practice and before and in some cases, even during wrestling matches.
But the disease is certainly not limited to high school athletics. In 2003, the St. Louis Rams had to disinfect their playing surface and their practice fields, following the revelation that opposing teams were contracting MRSA after playing the Rams in their domed stadium. In fact, the New England Journal of Medicine published a scientific paper on the outbreak, submitted by researchers from (among other entities) the National Center for Infectious Diseases and the Epidemic Intelligence Service, Division of Applied Public Health Training, Centers for Disease Control and Prevention. The abstract is located at: http://content.nejm.org/cgi/content/abstract/352/5/468 . It says, in part:
We conducted a retrospective cohort study and nasal-swab survey of 84 St. Louis Rams football players and staff members. S. aureus recovered from wound, nasal, and environmental cultures was analyzed by means of pulsed-field gel electrophoresis (PFGE) and typing for resistance and toxin genes. MRSA from the team was compared with other community isolates and hospital isolates.
During the 2003 football season, eight MRSA infections occurred among 5 of the 58 Rams players (9 percent); all of the infections developed at turf-abrasion sites. MRSA infection was significantly associated with the lineman or linebacker position and a higher body-mass index. No MRSA was found in nasal or environmental samples; however, methicillin-susceptible S. aureus was recovered from whirlpools and taping gel and from 35 of the 84 nasal swabs from players and staff members (42 percent). MRSA from a competing football team and from other community clusters and sporadic cases had PFGE patterns that were indistinguishable from those of the Rams' MRSA; all carried the gene for Panton–Valentine leukocidin and the gene complex for staphylococcal-cassette-chromosome mec type IVa resistance (clone USA300-0114). (bold mine)
From the Bloomberg story of 2005:
Episodes of drug-resistant infections have occurred in the past year on professional U.S. football teams, including the St. Louis Rams, Baltimore Ravens, and San Francisco 49ers, said Dan Jernigan, chief of CDC's epidemiology branch at the National Center for Infectious Diseases. Infections have been seen among newborns in nurseries, he said.
In an article in today's Washington Post, reporter Rob Stein gives some unbelievable new factoids. http://www.washingtonpost.com/wp-dyn/content/article/2007/10/16/AR2007101601392.html?hpid=topnews
A dangerous germ that has been spreading around the country causes more life-threatening infections than public health authorities had thought and is killing more people in the United States each year than the AIDS virus, federal health officials reported yesterday.
The microbe, a strain of a once innocuous staph bacterium that has become invulnerable to first-line antibiotics, is responsible for more than 94,000 serious infections and nearly 19,000 deaths each year, the Centers for Disease Control and Prevention calculated.
MRSA is a strain of the ubiquitous bacterium that usually causes staph infections that are easily treated with common, or first-line, antibiotics in the penicillin family, such as methicillin and amoxicillin. Resistant strains of the organism, however, have been increasingly turning up in hospitals and in small outbreaks outside of heath-care settings, such as among athletes, prison inmates and children.
The CDC's Scott K. Fridkin discloses the results of a multi-state study of MRSA. It yielded the following information:
In the new study, Fridkin and his colleagues analyzed data collected in California, Colorado, Connecticut, Georgia, Maryland, Minnesota, New York, Oregon and Tennessee, identifying 5,287 cases of invasive MRSA infection and 988 deaths in 2005. The researchers calculated that MRSA was striking 31.8 out of every 100,000 Americans, which translates to 94,360 cases and 18,650 deaths nationwide. In comparison, complications from the AIDS virus killed about 12,500 Americans in 2005.
"This indicates these life-threatening MRSA infections are much more common than we had thought," Fridkin said.
In fact, the estimate makes MRSA much more common than flesh-eating strep infections, bacterial pneumonia and meningitis combined, Bancroft noted.
"These are some of the most dreaded invasive bacterial diseases out there," she said. "This is clearly a very big deal."
The infection is most common among African Americans and the elderly, but also commonly strikes very young children.
So there are more deaths from MRSA in the United States that there are from HIV/AIDS, a recognized pandemic. And perhaps MRSA is a candidate for true pandemic status, based on this snippet, also from the Bloomberg article of 2005:
The Netherlands has taken a ``search and destroy'' approach to drug-resistant superbugs, said Vincent Jarlier, an infection control officer for the Assistance Publique hospital network in France. Dutch doctors and nurses who test positive for the superbugs must have six negative tests before they can return to work, he said. Hospitals are required to shut down wards where the superbugs are detected; one hospital shut down ten at one time.
But wait, there's more! Vietnam has had its own MRSA epidemic. From the National Institute of Health, published just last month: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1950567
An Outbreak of Severe Infections with Community-Acquired MRSA Carrying the Panton-Valentine Leukocidin Following Vaccination
We carried out a field investigation after adverse events following immunization (AEFI) were reported. We reviewed the clinical data from all cases. S. aureus recovered from skin infections and from nasal and throat swabs were analyzed by pulse-field gel electrophoresis, multi locus sequence typing, PCR and microarray. In May 2006, nine children presented with AEFI, ranging from fatal toxic shock syndrome, necrotizing soft tissue infection, purulent abscesses, to fever with rash. All had received a vaccination injection in different health centres in one District of Ho Chi Minh City. Eight children had been vaccinated by the same health care worker (HCW). Deficiencies in vaccine quality, storage practices, or preparation and delivery were not found. Infection control practices were insufficient. CA-MRSA was cultured in four children and from nasal and throat swabs from the HCW. Strains from children and HCW were indistinguishable. All carried the Panton-Valentine leukocidine (PVL), the staphylococcal enterotoxin B gene, the gene complex for staphylococcal-cassette-chromosome mec type V, and were sequence type 59. Strain HCM3A is epidemiologically unrelated to a strain of ST59 prevalent in the USA, although they belong to the same lineage.
So while we all try to figure out what the heck H5N1 is doing, remember that the Devil you know -- MRSA -- is out there, multiplying, mutating and killing. Sometimes we'd prefer the Devil you know over the Devil you don't know.
An influential voice weighs in on pandemic preparedness
Scott McPherson
in Information technology, Politics and government, Popular Culture, influenza and infectious diseases
|
8 Comments
 Thomas P.M. Barnett has written an excellent opinion piece for the Scripps-Howard News Service. Titled "In the future: health screening at airports," the piece clearly and plainly lays out the enormous difficulties nations and the aviation industry in general will face when the next pandemic arrives (via a scheduled passenger airline flight). The link is at: http://www.scrippsnews.com/node/27573
Thomas P.M. Barnett has written an excellent opinion piece for the Scripps-Howard News Service. Titled "In the future: health screening at airports," the piece clearly and plainly lays out the enormous difficulties nations and the aviation industry in general will face when the next pandemic arrives (via a scheduled passenger airline flight). The link is at: http://www.scrippsnews.com/node/27573
Barnett is no stranger to planning. In fact, if you have not heard of him, let me condense his story. Barnett was in the Pentagon in the late 1980s and started giving Powerpoint presentations regarding what he believed was the inevitable implosion of the Soviet Union. He even went so far as to predict the American Navy, for example, would be called upon to help its Soviet counterparts.
The assembled admirals and generals scoffed at this heresy. More than once he was laughed out of the room. But the ensigns, commanders and captains in the back rows -- the inheritors of the military after the current silver-hairs retired -- they listened with intense interest.
And they believed.
 When the Soviet Union did collapse, just as Barnett predicted and within the timeframes predicted, and the U.S. was asked to help its former enemies, those same youthful military leaders sought out the visionary Barnett. "Where's that guy with the Powerpoint!" they would yell at their adjutants. In response, Barnett's first book -- The Pentagon's New Map -- was a New York Times bestseller and the second-most popular book in the entire Pentagon, behind the Bible. Barnett's follow-up work, A Blueprint for Action, also sold well and both books are in trade paperback today and available at fine bookstores across the United States.
When the Soviet Union did collapse, just as Barnett predicted and within the timeframes predicted, and the U.S. was asked to help its former enemies, those same youthful military leaders sought out the visionary Barnett. "Where's that guy with the Powerpoint!" they would yell at their adjutants. In response, Barnett's first book -- The Pentagon's New Map -- was a New York Times bestseller and the second-most popular book in the entire Pentagon, behind the Bible. Barnett's follow-up work, A Blueprint for Action, also sold well and both books are in trade paperback today and available at fine bookstores across the United States.
He is also a buddy of mine, so I am happy to shill for him! Barnett gives the most lucid explanation for the violence directed against the civilized world today via his "Core and Gap" message. It is simple yet not simplistic. It is simple genius and one only wishes someone at 1600 Pennsylvania Avenue would stand up and articulate it to the world. He is frequently bookended in peoples' minds with fellow globalization maven Thomas Friedman. To contrast: Friedman is the diplomat and Barnett is the enforcer (again, a reference to his desire to revamp the military into "The Leviathan" and "System Administrators" -- oh, just go buy the damn books!). He is sometimes described as "Jack Ryan with a Powerpoint." He is brilliant.
Barnett was heavily involved in the Pentagon's Y2K planning effort in the late 1990s, which is where I first heard of him. As I was running Florida's statewide Y2K preparedness effort, I naturally took a deep interest in those in Washington who were also thinking way outside the box.
Anyway, I have taken some excerpts from his latest column, which I referenced way back in the beginning of this blog. Here they are:
The White House recently released its new homeland security strategy and, unlike the initial 2002 version, this one focuses far more on natural disasters as opposed to terrorist strikes. That's a welcome change not simply because Hurricane Katrina was a humbling experience, but because globalization's growing connectivity means a naturally occurring pandemic is the most likely mega-disaster we'll face in the near term.
A bird flu-triggered pandemic could easily become the most deadly global outbreak since the 1918 Spanish Flu, which killed at least 20 million people worldwide. In the United States alone, over one-quarter of the population became sick, with approximately 600,000 people succumbing to the virus. Extrapolated to today's American population of 300 million, that yields a potential death count of 1.5 million to 2 million.
Flu strains enter the United States in the bodies of sick travelers, so the key here will be our efficient and effective screening of in-bound passengers at international airports. According to Oak Ridge National Laboratory scientists currently investigating pandemic response procedures for the Department of Homeland Security, for every flu carrier who --unwittingly or not-- eludes that envisioned net, as many as 10,000 Americans could suffer exposure within three weeks time.
Consider the sheer volume: over 25,000 passengers arrive through Los Angeles' international terminals on a daily basis. In August, when a software glitch struck U.S. Customs' computers there, 20,000 passengers were stranded for up to 18 hours.
Ideally, any systemic approach would include initial diagnostic screens conducted overseas at originating airports. Since virtually all international flights are lengthy, passive diagnostic screening at points of embarkation and debarkation would offer authorities the opportunity to compare and contrast readings over time. For example, additional measures would be warranted if a passenger's symptoms worsened during the flight or if those symptoms spread to other passengers.
In the summer of 2004 my wife and I got a preview of this sort of screening at Honk Kong's international airport during a localized outbreak of avian flu cases. As we walked through the terminal with our youngest child, just then adopted from China, I noticed a large computer screen along the wall where our ghostly images were being displayed in real time. It turned out that airport authorities were scanning our body temperatures passively as we passed through a chokepoint.
I walked over to the technicians and asked about the procedure, only to be told that if any of us had registered an above normal temperature, our entire family would have been required to spend at least 48 hours in Hong Kong -- at our own cost! -- before we could again attempt departure on an outbound flight. Fortunately for us, what turned out to be our infant daughter's impending ear infection didn't kick in fully until we were several hours into our cross-Pacific flight. Had we been again screened at our American port of entry, we would have been nabbed, preventing -- for all we knew at the time -- something far worse from unfolding. (bold mine)
Where do you draw the lines in all of this? I can't begin to say.
I just know it's important that our Department of Homeland Security think through all realistic scenarios and gear up for the real-world tests that inevitably lie ahead.
Thomas P.M. Barnett is a distinguished strategist at the Oak Ridge Center for Advanced Studies and senior managing director of Enterra Solutions LLC.
As fellow bloggers Crawford Kilian and Mike Coston have pointed out, it is refreshing to have someone actually use the correct numbers when predicting an influenza pandemic. It is no surprise that Barnett would use the appropriate numbers when predicting the potential pandemic's impact on the U.S. population.
What is most important to all of us is this: Because of Barnett's extreme gravitas inside and outside of the Pentagon and the Washington media, government think tanks and policy wonks everywhere, his voice becomes a powerful force for pandemic preparedness. I am hopeful that this is the first of many, many written and vocal forays into the world of pandemic preparedness. His Website/blogsite, by the way, is www.thomaspmbarnett.com .
It's not always influenza that kills
Scott McPherson
in influenza and infectious diseases
|
1 Comment
 While influenza hogs the world viral stage, adenovirus steals the show.
While influenza hogs the world viral stage, adenovirus steals the show.
One thing I have learned after a twenty-one month immersion into the world of influenza research is that you'd better be ready to learn a whole lot more about other illnesses. That lesson could not be made clearer than this week, when I began to learn about the adenovirus.
Last week ,reports began to filter out of Mexico and Panama of a "mystery illness" that was killing scores of children.
As reported in the Miami Herald, edited by me:
Mystery disease strikes remote area of Panama
Posted on Tue, Oct. 02, 2007
BY ERIC JACKSON
Special to The Miami Herald
PANAMA CITY, Panama -- Local officials are reporting that 42 people have died, almost all of them children, in an outbreak of a still unidentified disease in the remote Ñurum district of Panama's indigenous Ngobe-Bugle region.
The ailment begins with a runny nose, coughing and fever, and when it gets deadly the victims present symptoms that look like bronchial pneumonia, according to a statement by Panama's Health Ministry.
The Health Ministry and the semi-automomous Gorgas Memorial Laboratory say they don't know the cause of the illness.
''We're studying it, and the Gorgas Lab is working on it, but to say anything now would be speculation,'' said a ministry official who asked for anonymity because he lacked authorization to comment on the case.
Word of a problem first got out in mid-September when local officials contacted the Health Ministry and then, alarmed by what they considered a lackadaisical response, took their story to the news media.
On September 23 Gladys Guerrero, the ministry's director of epidemiology, denied to a reporter for the tabloid El Siglo that there was any viral or bacterial pathogen at work, attributing the problem to complications of rainy season colds that are common in the area, especially because of its poor sanitary conditions.
Guerrero also said that local claims at the time of 10 deaths since late August were exaggerated. Within five days, Ngobe officials were reporting 40 deaths and many more sick. The La Prensa newspaper has reported that more than 30 children from Ñurum are being treated in various hospitals around the country.
The Health Ministry said in a Sept. 29 press release that the problem appears to be ''a known acute viral respiratory situation like influenza,'' but on Monday a ministry spokesman said that no flu or other virus had yet been identified.
The U.S. government has offered help, but as of Tuesday Panama had not asked for international assistance.
After news of the illness broke, President Martín Torrijos cut short a trip to the United States and flew into Ñurum with a team of some 60 healthcare workers. (bold mine)
Government officials fanned out to visit thousands of families and advise them to cooperate with health officials and that nobody evacuated to a city hospital would be left stranded -- a concern that had led some of the poor parents to refuse to let their children be taken to a hospital.
http://www.miamiherald.com/news/brea...ry/258274.html
So the president of panama ended his Washington visit with President Bush so he could take command of the situation. That is telling. Now, we have confirmation that the virus is none other than -- adenovirus. From today's FluTrackers forum (edits by me), and a huge hat-tip to poster Dutchy:
Minister confirms deaths of Panamanian natives by adenovirus
Panama, 10 oct (PL) the minister of Panamanian Health, Rosario Turner, today confirmed the death of 17 smaller indigenous children of five years, victims of curable respiratory diseases that proliferate in the isolated region Ngobe Buglé.
In an appearance before the Commission of Health and Social Security of the National Assembly, Turner said that 93 members of the community were hospitalized and of them 77 withdrew after receiving the corresponding treatments.
Turner declared that the respiratory deaths and serious pictures that appeared the last weeks in the community of Ñurum, in the referred region, must adenovirus and influenza, (bold Dutchy) in as much discarded all possibility of a mortal germ.
Communitarian leaders said days back that at least 40 minors and an adult passed away of the attacks of cough, fevers and diarreas, but as many were buried near their houses, far from health facilities.
The holder of Health expressed that the problem must to a virus that affects to children and adults with nutricionales problems and of anemia, but that the fast action of the unfolded medical personnel in the region avoided new deaths.
Turner said that the arisen respiratory diseases in the indigenous community are own of the rainy station in the country reason why it reiterated to maintain the measures of personal hygiene.
http://www.prensa-latina.cu/article....7d&language=ES
By itself, this article would not amount to too much. But let's seek context, and rewind two weeks ago to this report from Mexico, courtesy of WorldNetDaily:
Dozens in Mexican city ill with suspected avian flu
Raises concerns over international implications of epidemic
September 28, 2007
© 2007 WorldNetDaily.com
Dozens of people in a Mexican city are gravely ill with what is being treated as a possible outbreak of avian flu, according to a new report from a Spanish-language website.
According to El Universal, authorities in a neighborhood in Guanajuato say 45 patients have been given medical attention at the area's hospital after they reported symptoms including extreme headaches, stomachaches, vomiting and diarrhea.
The cases have developed over the last two weeks and "feel [like] death," according to Silvia Villalobos, one of the victims who spoke to El Universal correspondent Xochitl Alvarez in Spanish.
A spokesman for the regional general hospital, Ernesto Castle, said he does not know the cause of the problems, but officials are looking at an avian flu virus, which is transmitted by birds and is similar to botulism, as a source.
He reported at least 45 patients have been given emergency room medical attention, while others went to their private physicians for help.
One man reported his wife was hospitalized after the symptoms hit, waking her with fever and chills, before she fainted.
Guadalupe Gomez, a resident of the area, said her concern was that the epidemic was being carried by flies attracted by leather processed in the tanning industry, which includes leathers from other nations.
City spokesman Jose Eusebio Olague said officials have directed that barricades be set up so the sick do not spread the infections even further.
Traditional causes for fever and chills essentially have been ruled out by various tests, officials said. Sources in the air, water and other industries have been eliminated as a cause, officials said.
I will bet a dollar the Mexican virus is adenovirus.
Coincidentally, or perhaps serendipituously, a report was just issued this week on adenovirus 14 (oh, THAT adenovirus!).
IDSA: Outbreak of Severe Pneumonia Traced to Adenovirus 14
SAN DIEGO, Oct. 9 -- A potentially deadly form of community-acquired pneumonia linked to adenovirus type 14 has emerged in the Pacific northwest, according to a report presented here.First encountered in 2005 in Oregon, the viral pneumonia frequently leads to hospitalization and has a 20% fatality rate, (bold mine) Paul Lewis, M.D., of the Oregon State Public Health Department, said at the Infectious Diseases Society of America meeting.
"We recommend obtaining a viral culture in pneumonia patients who lack a specific etiology, especially those with severe disease," said Dr. Lewis. "If adenovirus 14 is detected, anticipate a stormy course. We encourage an infectious disease consultation to discuss the risks and benefits of any specific therapy that might be contemplated."
Recognition of the adenoviral pneumonia began with four patients hospitalized simultaneously at a Portland hospital. Upon comparing notes with physicians at area hospitals, Dr. Lewis and colleagues "almost fell out of our chairs because every hospital we called had recent severe and fatal cases of adenovirus disease."
(ditto) Investigators followed up the informal communication with a systematic review of all cases of adenovirus disease identified by Oregon clinical laboratories from November 2006 to April 2007. Six months of active surveillance revealed what appeared to be a winter-spring predominant adenovirus disease, as the number of reported cases increased from January through April.
Isolates from the sickest patients were sent to the CDC, which found that almost all the cases involved adenovirus 14, a serotype identified more than 50 years ago but rarely detected since then and never in association with outbreaks.
Dr. Lewis and colleagues at the state health department reviewed analyzed specimens dating back to 1993 and found a few cases of adenoviral disease almost every year. Beginning in 2005 adenovirus 14 was the predominant serotype identified.
Comparison of 31 patients with adenovirus 14 disease and 14 patients with other adenovirus serotypes showed that adenovirus 14 tended to infect older men (median age 52.9), and almost half the cases involved smokers. Most strikingly, adenovirus 14 was associated with a hospitalization odds ratio of 15.9 compared with other adenovirus serotypes.
The most common clinical features leading to diagnosis of adenovirus 14 disease were fever (~80%), tachypnea (75% to 80%), hypoxia (~50%), and hypotension (40% to 45%). Chest x-rays were abnormal in 23 of 24 cases. Radiographic progression was common, including single-lobe disease to multilobe in 55% of cases and lobar disease to adult respiratory distress syndrome in 45%.
All patients received broad-spectrum antibiotics. Dr. Lewis said 22 of the 31 patients with adenovirus 14 disease were hospitalized, and 16 required ICU care. Median hospital and ICU length of stay was seven days. Of the patients treated in the ICU, 13 required ventilatory support and eight had severe hypotension requiring pressor drugs. Seven patients (22%) died.
Risk factors for death or ICU care were a creatinine level greater than 1.2 mg/dL, lymphocyte count less than 100 µL, and coinfection with another pathogen. None of those factors remained statistically significant in multivariate analysis.
"This came out of nowhere in 2005 in Oregon," said Dr. Lewis. Acknowledging that almost all of the cases have involved severe illness, he agreed that the scope of the problem could be much larger and involve a broader spectrum of illness severity.
I don't know about where you live, but here in Tallahassee, we have been hit with what appears to be an epidemic of pneumonia. I personally know several people who were diagnosed with "viral pneumonia." I had a terrible cold with severe chest congestion last month that nearly sent me to the hospital and recently floored my wife as well. I am betting that where you live, you too had an experience similar to mine.
SARS was/is/will be again, a coronavirus that normally is associated with the common cold. Only in 2003, in China, this cold virus jumped species and mutated into a respiratory illness with a 10% case fatality rate. So what is to stop a mutant strain of adenovirus from growing in the jungles and rain forests of Central America and emerge on the world scene, as SARS emerged from the jungles of Southeast Asia?
Nothing. And, of course, there is no vaccine for adenovirus.
The CDC definition of adenovirus can be found at this link: http://www.cdc.gov/Ncidod/dvrd/revb/respiratory/eadfeat.htm . It says, in part:
Adenoviruses most commonly cause respiratory illness; however, depending on the infecting serotype, they may also cause various other illnesses, such as gastroenteritis, conjunctivitis, cystitis, and rash illness. Symptoms of respiratory illness caused by adenovirus infection range from the common cold syndrome to pneumonia, croup, and bronchitis. Patients with compromised immune systems are especially susceptible to severe complications of adenovirus infection. Acute respiratory disease (ARD), first recognized among military recruits during World War II, can be caused by adenovirus infections during conditions of crowding and stress. (bold mine).