
Entries by Scott McPherson (423)
Thinking the unthinkable: Asymptomatic or Airborne Ebola in Uganda?
 Scott McPherson
in influenza and infectious diseases
|
Scott McPherson
in influenza and infectious diseases
|
 2 Comments
|
2 Comments
|
 1 Reference
1 Reference
 Something is going on in Uganda, and it is causing health care workers to flee in panic.
Something is going on in Uganda, and it is causing health care workers to flee in panic.
First, some background on the current outbreak, from Reuters:
Death-toll rises from Uganda's Ebola outbreak
Sat Dec 1, 2007 10:43 AM ET
By Francis Kwera
KAMPALA (Reuters) - Two more Ugandans have died of a new strain of the deadly Ebola virus in an outbreak near the border with Democratic Republic of Congo, bringing the death-toll to 18, health officials said on Saturday.
"We have had two more deaths in the last 24 hours, and the disease continues to spread," Sam Zaramba, the Ugandan Health Ministry's director of health services, told Reuters.
Zaramba said World Health Organization (WHO) officials had teamed up with local experts to draw up a strategy to contain the outbreak of the hemorrhagic fever in the western Bundibugyo region. More than 50 people are also infected.
"We have set up isolation wards where all those who have been diagnosed with Ebola have been quarantined, and are being monitored closely," Zaramba added.
Genetic analysis of samples taken from some of the victims shows it is a previously unknown type of Ebola, making it the fifth strain, U.S. and Ugandan health officials say.
Ebola can cause internal and external bleeding. Victims often die of shock, but symptoms can be vague, including fever, muscle pain and nausea. It is known to infect humans, chimpanzees and gorillas.
Uganda was last hit by an epidemic of Ebola in 2000, when 425 people caught it and just over half of them died.
An outbreak in neighboring Congo this year infected up to 264 people, killing 187, the World Health Organization says.
Ugandan health officials originally suspected Marburg, a close Ebola cousin that infected three people in a different part of western Uganda the month before, killing one.But samples had tested negative.
(Writing by Andrew Cawthorne; Editing by Michael Winfrey)
Now, we get the "boots on the ground" view, from FOCUS Information Agency:
Kampala. Several dozen medics and support staff have fled western Uganda after their coworkers became infected with the Ebola virus in an outbreak that has already killed 18 people, officials said Saturday.
Ugandan officials clamped a quarantine on the Bundibugyo region and appealed for help in dealing with the outbreak of Ebola, a contagious disease that kills up to 90 percent of those infected, AFP reported.
However efforts to contain the outbreak, which began in September but was definitively identified as Ebola only last week, have been hampered by medical personnel becoming infected and others fleeing.
"We have a shortage of health workers and we need more because those who were there on the ground have been infected: two doctors, a medical officer and a nurse," said Sam Zaramba, the country's top government physician.
"Health workers are terribly afraid. They have abandoned patients in health units for fear of being infected," a government official told the state-owned New Vision newspaper.
There is a theory among microbiologists -- not much more than that, but a theory nonetheless -- that in order for a lethal disease to proliferate, it must reduce its lethality in order to spread more easily. We have discussed this time and again regarding the case fatality rate for H5N1. We have discussed this on this Blogsite. Could there be some kind of counterbalance in Nature, a biological "haggling session" that allows diseases to become more widespread in exchange for a reduction in lethality?
If these forces are at work in Uganda today, they may have produced a mutation that is less deadly yet much more easily transmitted. With the apparently easy transfer of what I will christen Ebola Uganda to health care workers, enough to cause a stampede out of the affected region, we should be very concerned.
Easy transfer? Since the outbreak was discovered in September, health care officials originally suspected Marburg virus, a hemorrhagic cousin of Ebola, they would have used protocols similar to those of Ebola. They are or should not be surprised by the diagnosis of Ebola, since much of sub-Saharan Africa has seen outbreaks over the years.
So what would cause them to flee in panic? How about Ebola that defies protocols and may actually be airborne or transmitted by asymptomatic human carriers?
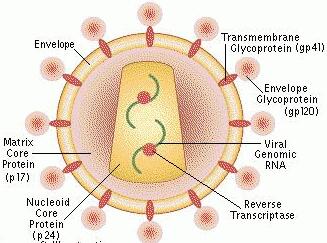
I found a nifty, short description of the four previously known strains of Ebola from the Website of one Bret Russell (http://www.brettrussell.com/personal/what_strains_exist_.html
- Ebola Zaire - The virus discovered in Zaire in 1976 - the first known occurrence of the Ebola Virus.
- Ebola Sudan - Initially discovered in western Sudan in 1976. This type of Ebola virus resurfaced again in 1979 in Sudan.
- Ebola Reston - This is the variation of the Ebola virus discovered in the African monkeys imported to the United States. This particular type is not believed to cause health problems in Humans.
- Ebola Tai - This is the most recently discovered type of the Ebola virus. Discovered in 1995 on the Ivory Coast of West Africa, in the Tai Forest. A Swiss researcher was the first infected human, but survived the infection.
Ebolas Zaire, Sudan, and Tai cause illness in humans as well as primates (monkeys). Ebola Reston does not cause illness in humans, but does cause illness in monkeys. Ebola Reston is suspected to be airborne (transmitted by the air) where the other strains are not transmitted by air. As for their structure, they are all quite similar in (string-like) shape, but have different gene sequences in places, and therefore different properties.
 Note that Ebola Reston is named after the city of Reston, Virginia -- site of the book "The Hot Zone." Its origin appears to be from the Philippines, since that is where the imported infected monkeys came from.
Note that Ebola Reston is named after the city of Reston, Virginia -- site of the book "The Hot Zone." Its origin appears to be from the Philippines, since that is where the imported infected monkeys came from.
While trolling the Internet on the subject of potential airborne transmission of Ebola, I found an interesting article from a biology student at Bryn Mawr University Jennifer L. Wilson. Ms. Wilson writes:
Secondly, one must consider epidemiological factors. For a major epidemic of the virus, conditions include: " Presence of the animal or insect vectors, whatever they may be, in proximity to a human population; 1) exposure of even a single infected human to others, by traveling from a remote setting, to a population center after exposure to a vector and/or reservoir in that remote setting; 2) deficient sanitation and hygiene among the population (lack of clean water supplies, sewage disposal & treatment, etc.) which increases the chance of bodily fluid contact (e.g., contact with fresh sewage containing wastes from Ebola victims); 3) decreased immune response in members of the population, whether from malnutrition or other disease burdens, especially AIDS; 4) social customs which increase bodily fluid contact between people (e.g., burial customs, multiple-partner sex); 5) inadequate public health infrastructure (hospitals, staff, equipment - e.g., enough syringes to prevent their re-use, isolation facilities, barrier supplies); 6) lack of awareness of the disease and its symptoms among the population; 7) access to transportation systems; 8) poor communications infrastructure, resulting in delays in medical response and public notification & education; 9) the mutation of Ebola so that a strain that is dangerous to humans becomes airborne." (12) While the last condition is currently not an issue, it is also the most grave of the conditions, and would allow an epidemic of the Ebola virus to reoccur in vast proportions. Furthermore, it may be assumed that airborne transmission is the best possible trait for the virus, as a mutation of this degree would ensure its continued evolution and progression.
Many Ebola researchers believe that apes are simply a short-term vector of the disease, and that the ultimate host is unknown but could be something along the lines of a tick or other small, pesky insect. Otherwise, they postulate, how could Ebola ever continue to exist? If apes die from Ebola (and certain African gorillas are now in danger of extinction because of Ebola), then how could they possibly be the long-term host?
So, while trolling the Net, you can imagine my surprise as I came across a Website dedicated to the Bible Code. I am fascinated by such attempts to prove prophecy, so I throw this in just to entertain and enlighten. Anyway, a gentleman found this passage at the intersection of a few Hebrew letters:
It may indicate a major Ebola epidemic in year 2007-2010.... The next two matrices are from a -300,000 to 300,000 Old Testament search for ARTHROPOD and EBOLA, since Arthropods are the family of animal life that includes ticks, mites, spiders, and insects, which are possible Ebola vectors. So we will try to see if an Arthropod is the Ebola vector host.
God, I love this stuff. The Website is located at: http://www.angelfire.com/zine2/Number666/KingJames10.html
Turning back to science, I found a 2003 Powerpoint from one Risha Patel, hosted by the University of Southern California (Go Trojans!). Patel's presentation also mentions possible permanent reservoirs of Ebola, including bats, plants, arthropods. Patel further writes that the "Wide range of potential reservoirs makes identification more difficult." Further trolling confirms the potential for insects and bats to transmit Ebola and Marburg. And just this past August, researchers at the Centers for Disease Control and Prevention (CDC), Atlanta, GA, and the Centre International de Recherches Médicales de Franceville (CIRMF) and the Institut de Recherche pour le Développement, Franceville, Gabon, confirmed the presence of Marburg in African fruit bats, so one vector has now been proven.
Patel's presentation can be viewed at: bioweb.usc.edu/courses/2003-spring/documents/bisc419-r.patel.ppt .
Question of the Millennium: If Reston Ebola can be considered airborne, even though it only impacts apes, could a new, previously undetected strain of Ebola "go airborne and become a flyer?"
Stranger things have happened.
Giving the "other side" an opportunity to weigh in, I deliver the rebuttal: An article from Probe, the Columbia University journal. Titled "Airborne Ebola? A theory that won't fly," the article's author, David R. Zimmerman, is an adjunct professor at the Columbia Graduate School of Journalism and is the editor of Probe, a newsletter of science and media criticism. He writes:
Popular culture has a recurrent fascination with doomsday pathogens. Michael Crichton's The Andromeda Strain was a classic incarnation of this scary scenario.... In Richard Preston's book The Hot Zone and the film "Outbreak," we're frightened by real viruses, specifically Ebola.... The ostensibly responsible media are not immune to the temptation to stir these fears. In a May 12 editorial, the New York Times declared: "A modest genetic change might enable Ebola to spread rapidly through the air..."
That very same day, in the news section, Times reporter Lawrence K. Altman, M.D., handled the matter more soberly. Reporting from the Centers for Disease Control and Prevention in Atlanta, he wrote, "The deadly Ebola virus continues to spread in Zaire, chiefly affecting health care workers... [It] apparently spread initially among [doctors] and nurses who operated on a patient in Kikwit." Dr. Altman, an infectious-disease specialist who once worked at the CDC, added, "Transmission presumably was through contaminated blood..."
Can a bloodborne or body fluid-borne virus be transformed by a single mutation into an airborne agent (a "flyer"), as the scare scenarios imply? It's conceivable. But it's "probably unlikely," according to virologist Beth Levine, M.D. , director of virology research in the infectious diseases division at Columbia University's College of Physicians and Surgeons. "Single amino acid mutations can change the tropism [the residential preference] of a virus" in some experimental situations, Dr. Levine says, "but there haven't been any examples of such mutations actually occurring in nature, changing a virus from a bloodborne or bodily fluid route of transmission to a respiratory route."
So, says Dr. Levine, "The media's claim is not totally without scientific basis. But there are no precedents for it, and it's unlikely.
"I think it's irresponsible to raise that concern," she added, "because in general viruses are very well-adapted to their milieuand they don't just suddenly change their environment." Will this kind of level-headed assessment quell media hysteria? Stay tuned.
Indeed, stay tuned.
Finally, from Florida1, the founder and president of FluTrackers: A Lancet journal article from 2000, presenting very persuasive evidence that there are human asymptomatic carriers of Ebola. There are people who apparently are immune from the effects of the worst disease you can think of.
The Lancet 2000; 355:2210-2215
DOI:10.1016/S0140-6736(00)02405-3
Human asymptomatic Ebola infection and strong inflammatory responseDr EM Leroy DVM  a
a  , S Baize PhD a, VE Volchkov PhD b, SP Fisher-Hoch MD c, M-C Georges-Courbot MD a, J Lansoud-Soukate PhD a, M Capron PhD d, P Debré MD e, JB McCormick and AJ Georges MD a
, S Baize PhD a, VE Volchkov PhD b, SP Fisher-Hoch MD c, M-C Georges-Courbot MD a, J Lansoud-Soukate PhD a, M Capron PhD d, P Debré MD e, JB McCormick and AJ Georges MD a
SummaryBackground
Ebola virus is one of the most virulent pathogens, killing a very high proportion of patients within 5–7 days. Two outbreaks of fulminating haemorrhagic fever occurred in northern Gabon in 1996, with a 70% case-fatality rate. During both outbreaks we identified some individuals in direct contact with sick patients who never developed symptoms. We aimed to determine whether these individuals were indeed infected with Ebola virus, and how they maintained asymptomatic status.
MethodsBlood was collected from 24 close contacts of symptomatic patients. These asymptomatic individuals were sampled 2, 3, or 4 times during a 1-month period after the first exposure to symptomatic patients. Serum samples were analysed for the presence of Ebola antigens, virus-specific IgM and IgG (by ELISA and western blot), and different cytokines and chemokines. RNA was extracted from peripheral blood mononuclear cells, and reverse-transcriptase-PCR assays were done to amplify RNA of Ebola virus. PCR products were then sequenced.
Findings
11 of 24 asymptomatic individuals developed both IgM and IgG responses to Ebola antigens, indicating viral infection. Western-blot analysis showed that IgG responses were directed to nucleoprotein and viral protein of 40 kDa. The glycoprotein and viral protein of 24 kDa genes showed no nucleotide differences between symptomatic and asymptomatic individuals. Asymptomatic individuals had a strong inflammatory response characterised by high circulating concentrations of cytokines and chemokines.
Interpretation
This study showed that asymptomatic, replicative Ebola infection can and does occur in human beings. The lack of genetic differences between symptomatic and asymptomatic individuals suggest that asymptomatic Ebola infection did not result from viral mutations.
Elucidation of the factors related to the genesis of the strong inflammatory response occurring early during the infectious process in these asymptomatic individuals could increase our understanding of the disease. (bold Sharon's).
Airborne? Or asymptomatic? Whatever the situation, or the cause, the situation is rapidly devolving in Uganda. Now MSF, home to Ebola worker Zoe Young, has been called in. We will see what transpires.
Will Bali global warming summit be upstaged by disease?
 By now, everyone in the global warming and Flublogia communities knows about the global warming summit taking place as I write this blog, in Bali, Indonesia.
By now, everyone in the global warming and Flublogia communities knows about the global warming summit taking place as I write this blog, in Bali, Indonesia.
Of course, we Flubloggers have been taking the same approach regarding the location that horror movie fans take when watching victim after victim descend darkened stairs to investigate the curious noise emanating from the basement: "DON'T GO DOWN THERE! DON'T GO IN THE BASEMENT!"
But they go in the basement anyway, and we know that if they didn't, then gratuitous film violence and dismemberment would not happen. And so it is with the Bali summit: They have to go, even in the face of possible danger. They made the deal, and it is too hard to change locations, let alone cancel the event.
What danger, you ask? The danger of avian influenza. And apparently it is not as far-fetched as we might think. Currently, on FluTrackers, a thread is discussing the death last week of a Jakarta police commander on loan to the UN to help deal with security for the Bali summit. He died suddenly and, so far, inexplicably, from "difficult flu." He simply went to bed and died overnight. He died in the Bali capital of Denpasar. From flusite poster Dutchy, via machine translation:
The guard of the Conference UN Died because of Flu
Denpasar, on Tuesday - Brigadier Samsul Bahri (32), the member Traffic Police Greater Jakarta Metropolitan Regional Police died as a result of being attacked by acute flu. Samsul at this time was in-BKO-would as pengaman Konfereni UN about the Change in the Climate (UNFCCC) Denpasar, Bali.
"From results" of the "team's inspection" of the "doctor, Samsul it was mentioned died as a result of being attacked by difficult flu, not resulting from the existence" of the "criminal action," said Kasubid Humas Regional Police Bali AKBP Sri Harmiti, in Denpasar, on Tuesday (27/11).
Brigadier Samsul since several days ago was in Bali related UNFCCC security efforts, on Monday (26/11) at dawn around struck 02,00 Wita was found by his room-mate in the Hotel of Orange-Jee in Street Hayam Wuruk, Denpasar already in the situation died. When his room-mate came, said Sri, casualties Samsul were found died with the stiff body on his bed.
Saw that, the friend a room of casualties immediately reported to Regional Police Bali that afterwards entered carried out investigation. Kasubid Humas mentioned, the official of the investigator who was accompanied by the team of the doctor who carried out investigation, in his conclusion said that casualties were killed as a result of being attacked by quite difficult flu.
Along with that, the official who carried out investigation also did not find the guidance if the member Traffic Police Greater Jakarta Metropolitan Regional Police died resulting from the existence of the criminal action. After being checked, said Sri, in the afternoon same the Samsul body was despatched to Jakarta, to be handed over to the family.
(ANT/ABI)
http://kompas.com/ver1/Nusantara/0711/27/151516.htm
Nature is full of cruel ironies -- as displayed by, among other incidents, the recent sinking of a cruise ship down in Antarctica. The irony is the ship was a global warming cruise, and the ship/line is allegedly owned by a friend of Al Gore. The purpose of the cruise, I assume, was to investigate the melting of the Antarctic ice shelf. The ship hit an iceberg (!) and sank. All hands were saved, but imagine the pollution from the ship's bilges, fuel, oil, flotsam and jetsam, etc.
Imagine if the world's leaders gathered to debate an environmental event and wound up helping transmit a lethal disease all over the world? Stranger things have happened.
And since the lid will be welded shut on such reports while the Bali summit is taking place (and maybe well afterward), we may never know the true reason for the death of Jakarta Brigadier, Samsul Bahri.
What Momma taught us -- NOT Tamiflu or vaccine -- will save the most lives in a pandemic
Scott McPherson
in Politics and government, influenza and infectious diseases
|
Post a Comment
|
2 References
 A new report -- the culmination of surveying some 51 other medical reports and historical journals -- says that hand washing, proper hygiene, personal protective equipment and "doing what Momma taught us" will save the most lives in the civilized world once a pandemic arrives.
A new report -- the culmination of surveying some 51 other medical reports and historical journals -- says that hand washing, proper hygiene, personal protective equipment and "doing what Momma taught us" will save the most lives in the civilized world once a pandemic arrives.
The report, summarized in this US News and World Report story, can be found at this link: http://health.usnews.com/usnews/health/healthday/071129/handwashing-masks-beat-drugs-at-fighting-flu.htm
Handwashing, Masks Beat Drugs at Fighting Flu
Data review finds they're best at keeping individuals safe
THURSDAY, Nov. 29 (HealthDay News) -- When it comes to fighting the spread of influenza and other respiratory viruses, physical barrier measures -- such as handwashing and wearing masks, gloves and gowns -- may be more effective than drugs.
That's the conclusion of new research by experts who reviewed 51 published studies on the topic.
While many nations are stockpiling antiviral drugs to prepare for a possible future flu pandemic, there's increasing evidence that such drugs and vaccines won't be sufficient to block the spread of a major outbreak, noted a team led by Chris Del Mar of the faculty of health sciences and medicine at Bond University, Gold Coast, Australia.
On the other hand, there's clear evidence of a link between personal and environmental hygiene and infections, the researchers said. However, until now, there haven't been any comprehensive reviews of this evidence.
The studies examined by the review authors compared interventions to prevent viral animal-to-human or human-to-human transmission of respiratory viruses -- isolation, quarantine, social distancing, barriers, personal protection and hygiene -- to other kinds of interventions or to doing nothing. These studies did not include antiviral drugs or vaccines.
Handwashing and wearing masks, gloves and gowns were effective individually in preventing the spread of respiratory viruses, and were even more effective when all three were used in combination, the review authors found. Combining these measures may be more effective than antiviral drugs in fighting a pandemic, they said.
The review was published online Wednesday in the British Medical Journal.
Readers of this column know that I have been preaching this for months. The quick summary is that a vaccine, if ever effective at all, will not arrive until the Second Wave of a pandemic. So the First Wave of 8-12 weeks will already have happened, and a significant portion of the Earth's population will already be immune to the virus, strong drift and/or shift notwithstanding. And there are just not enough antivirals to go around; and Los Alamos even says that antivirals such as Tamiflu only forestall the pandemic; it will not eliminate it, according to supercomputer-driven exhaustive scenario after scenario.
So what Momma taught us, plus the application of PPEs and Non-Pharmeceutical Interventions, are our best hope for saving lives and delaying a pandemic. Government and corporate leaders would do well to heed this advice and do the following:
1. Stockpile the cheaper solution: masks, gloves, hand sanitizer, cleaning supplies and disinfectants.
2. Stockpile knowledge: Teach people to wash their hands, sneeze correctly, cough properly, and how to clean up after themselves.
3. Teach janitorial concerns how to clean hard surfaces -- and how NOT to vacuum in a pandemic.
4. Remind everyone what Momma taught us: Wash your hands, exercise proper hygiene, and keep a respectable distance from strangers.
5. Begin this TODAY, when the ROI from such matters can be applied to seasonal flu and other maladies.
We need to shift this debate away from stockpiling antivirals and toward doing the things we know we can do and the things we know we can count upon. You want a quick way to double antirivals? Stockpile cheap, plentiful Probenecid and administer it alongside Tamiflu (see my earlier posts and Google "probenecid" as well).
Why telecommuting will probably fail in a pandemic, Vol. 1
Scott McPherson
in Information technology, Politics and government, Popular Culture, influenza and infectious diseases
|
Post a Comment
|
2 References
 Has anyone noticed their Internet connection slowing down over the past few days?
Has anyone noticed their Internet connection slowing down over the past few days?
Has anyone not noticed the slowness of the Internet, especially at night?
E-commerce retailers are experiencing a huge surge in shoppers this holiday season. And nowhere is this more evident than in the (in)ability of users to expeditiously shop on their favorite Websites this holiday season. I can speak directly to this issue. For example, while shopping for a new television set online, I was thrown off Sears.com several times, and thrown off circuitcity.com almost as many times. Screen refreshes were agonizingly slow, and I would up shutting off the computer and waiting for a more suitable time to shop.
Welcome to the New Normal on the Internet once a pandemic starts. As we have discussed before, the New Normal (at least for 8 to 12 weeks at a time) will be socially-distanced parents attempting to work from home, while their kids are toiling away on their XBox 360s hooked up to the net, gaming with 200,000 of their closest online friends. The cumulative effect of this will be to slow even the highest-speed cable connection to a veritable crawl.
But even a pandemic may not be the trigger to bring the Web to its knees. A recent USA Today article speaks of the dangers to bandwidth that are just a few years off, even without the threat of a looming pandemic. Here it is:
Video, interactivity could nab Web users by '10
NEW YORK — Enjoy your speedy broadband Web access while you can.
The Web will start to seem pokey as early as 2010, as use of interactive and video-intensive services overwhelms local cable, phone and wireless Internet providers, a study by business technology analysts Nemertes Research has found.
"Users will experience a slow, subtle degradation, so it's back to the bad old days of dial-up," says Nemertes President Johna Till Johnson. "The cool stuff that you'll want to do will be such a pain in the rear that you won't do it."
Nemertes says that its study is the first to project traffic growth and compare it with plans to increase capacity.
The findings were embraced by the Internet Innovation Alliance (IIA), a tech industry and public interest coalition that advocates tax and spending policies that favor investments in Web capacity.
The findings were embraced by the Internet Innovation Alliance (IIA), a tech industry and public interest coalition that advocates tax and spending policies that favor investments in Web capacity.
"We're not trying to play Paul Revere and say that the Internet's going to fall," says IIA co-Chairman Larry Irving. "If we make the investments we need, then people will have the Internet experience that they want and deserve."
Nemertes says that the bottleneck will be where Internet traffic goes to the home from cable companies' coaxial cable lines and the copper wires that phone companies use for DSL.
Cable and phone companies provide broadband to 60.2 million homes, accounting for about 94% of the market, according to Leichtman Research Group.
To avoid a slowdown, these companies, and increasingly, wireless services providers in North America, must invest up to $55 billion, Nemertes says. That's almost 70% more than planned.
Much of that is needed for costly running of new high-capacity lines. Verizon is replacing copper lines with fiber optic for its FiOS service, which has 1.3 million Internet subscribers.
Johnson says that cable operators, with 32.6 million broadband customers, also must upgrade. Most of their Internet resources now are devoted to sending data to users — not users sending data. They'll need more capacity for the latter as more people transmit homemade music, photos and videos.
"Two years ago, nobody knew what YouTube was," Johnson says. "Now, it's generating 27 petabytes (27 million gigabytes) of data per month."
Schools, hospitals and businesses could add to the flood as they use the Web for long-distance education, health care services and videoconferencing.
Service providers might not appreciate how fast Web demand is growing, Johnson says: "Comcast doesn't know what's going on in AT&T's network, and vice versa. Researchers are increasingly shut out. So nobody's getting good, global knowledge about the Internet."
One of the best-kept secrets in netland is the existence of LambdaRail, an educational network that makes broadband seem as slow as dialup. First, some history: What we know today as the Internet was actually built by the US military during the Cold War. It was a data communications network called ARPANET; a network so resilient that it could survive multiple nuclear strikes. After the US military surrendered ARPANET to Higher Education, the colleges and universities turned it into what we know today as the Internet (sorry, Al, you didn't do a damn thing to build it). And then the planet took the Internet over from academia.
Academia never really got over that idea, so they built their own, faster, better net, called LambdaRail. It travels orders of magnitude faster than the public Internet does. And it has relatively few users; so few, in fact, that state university systems are now trying to resell LambdaRail bandwidth to anyone who technically qualifies (you have to have some serious jack, plus a smidgen of an educational purpose, so most need not even bother to apply). In my day job, I am seriously considering moving my organization to LR as a way to fuse our disaster recovery network planning with our daily net business model. If we move to LR, we hypothetically should avoid the wobbles, crunches and squeezes the rest of you peons will face when the pandemic arrives. HAHAHAHAAAAAAA!
Anyway, this LR stuff may all sound good, but the impact of a pandemic to global commerce, globalization itself, and the just-in-time economy will be sudden and devastating. The same Internet that carries your Flikr photos and YouTube videos also carries banking information, billions and billions of transactions, and literally trillions of dollars move on it annually. So the idea that during a pandemic, Johnny's game of Assassin's Creed for the 360, coupled with Mom's need to log in and hit the corporate mainframe via a Web portal cumulatively causing a global financial meltdown is more than just the stuff of fiction.
Booz Allen Hamilton came to this conclusion last June, when they predicted the Internet would collapse in the EU in Day Four of a severe pandemic. So the lesson is to watch the Internet this holiday season, study how it slows down, then envision this scenario being the New Normal during a pandemic. Or anytime in 2010, according to Gannett.
Happy shopping.
AIDS vaccine failure sends researchers back to Square One
Scott McPherson
in Politics and government, Popular Culture, influenza and infectious diseases
|
Post a Comment
 MSNBC has an excellent article today about the failure of Merck's AIDS vaccine and what it means to public health and medical research. Robert Bazell, NBC News's chief science and medicine correspondent, writes the following:
MSNBC has an excellent article today about the failure of Merck's AIDS vaccine and what it means to public health and medical research. Robert Bazell, NBC News's chief science and medicine correspondent, writes the following:
Indeed the vaccine development world is now in a state of stunned shock since the trial that many believed had the greatest chance of success was halted. At this point, it looks like an AIDS vaccine remains decades away, if one is ever to be found
Merck’s experimental vaccine did not simply fail to protect people. There were more infections among men who got the vaccine — 49 out of 914 — than those receiving a placebo — 33 of 922. There is no way the vaccine itself could have infected people. But the results raise the frightening prospect that the vaccine actually increased people’s chance of getting infected through sex or injection drugs. (bold mine)
“I don’t want to be Pollyanna and I don’t want to be Chicken Little. But we could have a very serious problem,” said Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases.
I found the following paragraphs to be interesting, if just coincidental, for the discussion of an old virus come back to haunt us -- adenovirus.
But what happened among the mostly gay male volunteers? Merck’s vaccine combined three proteins produced by the AIDS virus with a modified form of a virus that causes the common cold (adenovirus 5). (bold mine)
Preliminary analysis of the data finds that those who became infected with HIV mounted the strongest immune reaction to the adenovirus. This could be a fluke with this adenovirus. But it also could be something far more significant.
Bazell concludes his remarks with this paragraph:
But meanwhile we do know that treatment works well for those who are infected, and old-fashioned prevention efforts keep people from getting infected in the first place. Perhaps it is time to re-think the priorities. (bold mine)
HIV/AIDS is preventable. With the exclusion of those unfortunates who get infected unknowingly from spouses and partners who are unfaithful, or from tainted blood or organs, the application of simple common sense is a powerful agent against this pandemic disease.