
Entries in WHO (2)
How will we know if H7N9 establishes itself in the USA?
 Scott McPherson
in #H7N9, H5N1, H7N9, WHO, World health organization, avian influenza, bird flu, influenza and infectious diseases, pH1N1, pandemic, swine flu
|
Scott McPherson
in #H7N9, H5N1, H7N9, WHO, World health organization, avian influenza, bird flu, influenza and infectious diseases, pH1N1, pandemic, swine flu
|
 Post a Comment
Post a Comment
A few years ago, back in January 2009 (and six months before the swine flu pandemic), I wrote a blog regarding H5N1 and the potential for chickens to be asymptomatic carriers of a pandemic candidate virus.
If you performed a Find and Replace using "H7N9" for "H5N1" in that blog post, you would instantly have a very topical blog. So please read that blog from four years ago, and change the virus subtype in your head as you go along.
Now, I vector you to today's disclosure that 64 human H7N9 cases exist in six different provinces, including two fabled cases in the city of Beijing. There are 14 deaths. As I mentioned in one of my earliest blogs on the subject of human H7N9, barely a week ago:
Dr. Yin of the Bill and Melinda Gates Foundation. Apparently Dr. Yin is the Foundation's leader in China. And it was quite satisfying, knowing Bill and Melinda are spending funds in China, including, but not limited to, surveillance. Dr. Yin's statement is worth paraphrasing. He said, basically, if you don't test for H7N9, you won't find it. But if you do test for it, you'll find it. The inference is that there have been numerous unexplained and undiagnosed severe respiratory ailments there this season. Retroactive testing of samples, based on Dr. Yin's inference, will yield a significant increase in the number of H7N9 human cases.
Indeed, with more than 400 labs across China testing away, they are finding more cases in more geographic locations. Simultaneously, more deaths are being reported. Fortunately, the deaths are not increasing in proportion to the number of confirmed cases. We all believed that the case fatality rate would not be as high as the initial reports would have indicated; the sample was too low and the data, therefore, did not support (yet) a high CFR.
But I found it interesting that as of this morning, the WHO has not yet established a pandemic alert system for H7N9. Dedicated Web page, yes. But the WHO has not started an alert system.
WHO has an alert system in place for H5N1, and had one for pH1N1, a.k.a. The Virus Formerly Known As Swine Flu. Perhaps it is too early for such an alert system. After all, the virus is only in one region of one nation (albeit a region that is host to more than 300,000,000 Chinese). I also understand the reluctance the WHO must feel regarding this disease. The WHO took significant credibility hits after swine flu, some referring to the WHO as "chicken little." These criticisms are unfair and undeserved. No one had any idea that pH1N1 would have been as mild as it was.
And "mild" is a misnomer. The words "mild virus" are of great consolation to virus experts, public policymakers and public health professionals who look at The Big Picture; but those words are of little consolation to the parents of children who died during the pandemic.
A Reuters story from June of last year paints that smaller picture.
(Reuters) - The swine flu pandemic of 2009 killed an estimated 284,500 people, some 15 times the number confirmed by laboratory tests at the time, according to a new study by an international group of scientists.The study, published on Tuesday in the London-based journal Lancet Infectious Diseases, said the toll might have been even higher - as many as 579,000 people.
The original count, compiled by the World Health Organization, put the number at 18,500....
The results paint a picture of a flu virus that did not treat all victims equally.
It killed two to three times as many of its victims in Africa as elsewhere. Overall, the virus infected children most (4 percent to 33 percent), adults moderately (0 to 22 percent of those 18 to 64) and the elderly hardly at all (0 to 4 percent).
Even though the elderly were more likely to die once infected, so few caught the virus that 80 percent of swine flu deaths were of people younger than 65.
In contrast, the elderly account for roughly 80 percent to 90 percent of deaths from seasonal influenza outbreaks. They were probably spared the worst of 2009 H1N1 because the virus resembled one that had circulated before 1957, meaning people alive then had developed some antibodies to it.
The relative youth of the victims meant that H1N1 stole more than three times as many years of life than typical seasonal flu: 9.7 million years of life lost compared to 2.8 million if it had targeted the elderly as seasonal flu does."
So swine flu was much more of a force than anyone (especially the critics) thought it was.
Here in April of 2013, we have a big problem. No one knows how long this new H7N9 virus was circulating among wild birds, poultry and (especially) people in China. In fact, we didn't know Diddley until March 31st, when the Chinese sprung the news upon the world. Exactly when the Chinese knew it had H7N9 in people is cause for speculation, but I think we can excuse the Chinese for demanding confirmation before telling the whole world (to their credit) that a new pandemic candidate was emerging within their borders.
In fact, nothing may have ever been known, had the cases involving the three male family members not caused some doctor or technician to begin testing for something. My guess is they speculated it was seasonal influenza or H5N1 bird flu, then moved to SARS, then moved to the new novel coronavirus NCoV, and then reverse PCR testing revealed the presence of H7N9.
Thank the Maker that someone had the curiosity and the desire to test in a wider spectrum!
Adding to the drama is the report from Beijing last week that a 4-year-old boy tested positive for H7N9. He is not sick and displays no symptoms, yet he is an asymptomatic carrier of bird flu. This means wider testing is essential -- of humans, pigs and birds. The testing net needs to be cast very widely in order for everyone to get their arms around the problem.
And that, folks, is why I believe the USA's CDC opened its Emergency Operations Center at Level 2. Since the CDC EOC alert levels only go from 3 to 1, the opening at Level 2 was considered by some to be controversial.
Knowing now what we do, and analyzing their decision in the current light, we should say this was an important and prudent decision. Because, folks, we don't really know if this virus has come to America or not. And the only way we are going to know anytime soon is through weekly surveillance of mortality and morbidity.
From Wikipedia:
United States
On April 9th, 2013 the Centers for Disease Control and Prevention (CDC) activated its Emergency Operations Center (EOC) in Atlanta at Level II, the second-highest level of alert.[30] Activation was prompted because the novel H7N9 avian influenza virus has never been seen before in animals or humans and because reports from China have linked it to severe human disease. EOC activation will "ensure that internal connections are developed and maintained and that CDC staff are kept informed and up to date with regard to the changing situation."[31]
From the Medscape article:
The Centers for Disease Control and Prevention (CDC) in Atlanta, Georgia, received a specimen of the H7N9 virus from China yesterday. On April 9, the CDC activated the Emergency Operation Center (EOC) at Level 2 (there are 3 levels, with 1 as the highest) to support the management of the emerging H7N9 situation, Sharon KD Hoskins, MPH, senior press officer at the CDC told Medscape Medical News in an email.
Researchers used real-time reverse-transcriptase-polymerase-chain-reaction assays, viral culturing, and sequence analyses to test the patients' respiratory specimens for influenza and other respiratory viruses.
....In an accompanying perspective, Timothy M. Uyeki, MD, MPH, MPP, and Nancy J. Cox, PhD, from the Influenza Division, National Center for Immunization and Respiratory Diseases at the CDC, commented on the article, noting that this outbreak "is of major public health significance."
"The hemagglutinin (HA) sequence data suggest that these H7N9 viruses are a low-pathogenic avian influenza A virus and that infection of wild birds and domestic poultry would therefore result in asymptomatic or mild avian disease, potentially leading to a 'silent' widespread epizootic in China and neighboring countries," Drs. Uyeki and Cox write. The HPAI H5N1 virus usually causes rapid death in infected chickens.
I am not certain, but I am pretty confident that most labs in the United States are currently incapable of subtyping anything other than the prevaling seasonal flus of pH1N1, H3N2, B, and swine H3N2 (nice call, CDC). Anything other than these substrains are lumped into one or more catagories of A: "Subtyping not performed," or A "Unable to subtype." However, the CDC is also beginning to catalog incidences of other novel influenzas. From their April 6th report:
Assuming few, if any, US labs can currently quickly detect H7N9 bird flu, the only other capability the CDC has is to monitor and initiate surveillance of the public's health. This means both ramping up a central monitoring presence dealing with day-to-day issues, and also ramping up state health departments to begin watching for unusual spikes in ILI, or Influenza-Like-Illness.Novel Influenza A Virus
No new human infections with novel influenza A viruses in the United States were reported to CDC during week 14.
A total of 312 infections with variant influenza viruses (308 H3N2v viruses, 3 H1N2v viruses, and 1 H1N1v virus) have been reported from 11 states since July 2012. More information about H3N2v infections can be found at http://www.cdc.gov/flu/swineflu/h3n2v-cases.htm.
- By activating their EOC at level 2, the CDC is able to pull in disparate elements and to begin the process of surveillance in earnest. Things you just cannot do sitting at a desk, you can do in a central coordinating facility, open-air, with people at their posts. Having been in the State of Florida EOC many times, including pandemic exercises, actual hurricane tracking and the afternoon of 9/11 (and for days afterward), the ability to sort information and make decisions does not happen in a better environment.
On April 2nd, I formally activated the State of Florida CIO Association's Pandemic Committee. It had stood in informal recess since the Swine Flu pandemic was declared over in 2010. However, I decided that once the chickens were not doing their duty and dying, we had a real conundrum on our hands!
In fact, just last week, the Florida Department of Health announced that they were beginning monitoring the China H7N9 situation. I suspect other state health organizations are ramping up, if for no other reason than to give the CDC timely and accurate information, should there be spikes in respiratory illness.- So what would a spike look like? The spike would look something like this:
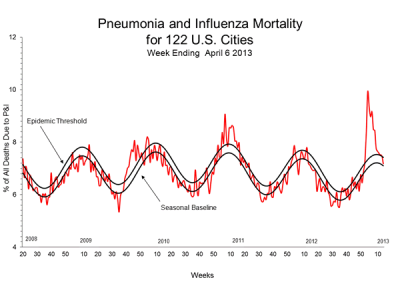
Hmmm. This is the actual CDC Pneumonia and Influenza Mortality chart for April 6th, 2013.
- The top black line represents the epidemic threshhold. The bottom black line represents the seasonal baseline.
- The red line represents the actual reported cases. As you can see, the red line is at the highest point since a spike at the beginning of calendar 2011, six months after the end of the Swine Flu Pandemic. In fact, the chart had suddenly spiked to a level higher than at any point since 2009.
- Not sure of what was going on, but knowing this occurred before my rebirth as a flu blogger, I reached out to Mike Coston (again). I asked Mike about what had happened?
- Mike told me that the CDC immediately looked into the situation. In fact, he blogged on both the mortality spike and the CDC's response. Apparently, what happened is that H3N2 drifted. If you need a primer on antigenic shift vs. antigenic drift, click here.
- Anyway, what happened is that, apparently, the H3N2 seasonal flu drifted. And seniors, who may not have been vaccinated as often as recommended, had no immunity to the drifted virus -- immunity they might have had, if they had goten regular flu shots. H3N2 is a nasty bug for anyone, but especially for the elderly, who died in numbers sufficient to trigger the uptick that you just saw.
- A similar uptick, especially coming now as flu season wanes, would trigger a pretty quick CDC response. This is why the CDC activated. This is why state departments of health are getting ready to ramap up their surveillance.
- To recap:
- The chickens are not doing their duty and dying.
- China has no real idea how widespread the virus is.
- Nobody else does, either.
- There is currently no reason to suspect there is H7N9 in North America.
- That having been said, there is always the possibility that infected, asymptomatic travelers have come into the United States via any of the Pacific ports of call and airports. Unlikely, but not impossible.
- Certainly, we would have seen the virus in Hong Kong before we would have seen it here.
- Currently, there is no inexpensive, routine way to test in doctors' offices or public health departments in the USA for H7N9.
- H7N9 would appear as "Type A, Unable to subtype" or "Type A, subtyping not performed."
- We have a long way to go with this situation.
Trust Fineberg's committee to deliver accurate, relevant, honest WHO appraisal
Scott McPherson
in H1N1, Harvey Fineberg, Politics and government, WHO, influenza and infectious diseases, pandemic, swine flu
|
Post a Comment
Wow. It has been more than two months since my last blog entry. that must mean that H1N1v, or swine flu, is gone, right?
No. It means I am incredibly busy these days, and have not had much to say about pandemics nor about infectious disease. Well, that is not entirely true. For example, dengue fever has established a beachhold in Key West, Florida, where a Navy person recently was confirmed to have contracted dengue from within Key West's city walls.
Also, and as most of us surmised, swine flu is still worming its way through the developing world. India seems to be under the gun with outbreaks of H1N1v, and I am not sure what the genetic makeup of this new virus might be.
Additionally, recent reports regarding testing of the H1N1 vaccine on mice and subsequent attempts at infection with 1918 Spanish flu are encouraging. It appears that there is some conferred immunity from the 1918 pandemic virus with the H1N1 swine flu vaccine. This is important, because if you recall from reading this Blog, the 1977 recurrence of H1N1 was believed to be the result of a Soviet lab accident. So this pandemic may have been serendipitous in that it is helping immunize the planet against another Spanish Flu.
Anyway, the article that prompted me to write this blog actually deals with the WHO analysis of itself. The WHO has been the subject of much scrutiny as the result of what has been to date, a very mild pandemic. Some are inferring that Big Pharma actually orchestrated this pandemic in order to make a lot of money on vaccine and antivirals.
Believe me, Big Pharma has more and bigger things to make money on than vaccines. Anyone who really believes Big Pharma would drop everything it was doing to go and make vaccine just does not understand how drug companies make their money today. Druf companies see vaccine production as a necessary evil; a component of what they do, but not nearly as profitable as making and selling drugs dealing with everything from erectile dysfunction to hair loss.
In fact, accusing drug makers of profiting unnecessarily from vaccine production may actually cause drug makers to forego vaccine production in the future. Now some, including those misguided but WRONG individuals who think vaccines cause autism, might rejoice in that thought. But the simple truth is that drug companies see vaccine production as an important public health duty. And accusing them of orchestrating an overly aggressive response to a flu pandemic is placing blame in the wrong place.
Is there a right place to place blame? In my opinion, no. There is no blame. The WHO acted correctly. Now there are protocol adjustments to make, and my previous blogs have covered the principal problems, dealing with severity. The WHO needs to adopt the US "Saffir-Simpson" standard for pandemic severity. I am sure that concept will get an airing and eventual adoption.
But the absolute best news I gleaned from today's article about the WHO oversight committee deals with the committee itself. First, the AP story of today:
2 experts resign from WHO swine flu review panel
(AP) – 1 hour ago
GENEVA — The World Health Organization said Tuesday that two members of an expert panel reviewing the global body's response to the swine flu outbreak have resigned over concerns about perceived conflict of interest.
John MacKenzie and Tony Evans stepped down because their close association with the UN health organization during the outbreak could be seen as conflicting with the panel's ability to remain independent, WHO said.
"Both have been closely engaged in deliberations at WHO which our committee is charged to review," said panel chairman Harvey Fineberg. "They each concluded it would be better to avoid the position as reviewer of their own earlier actions."
Mackenzie, a professor of tropical infectious diseases at Curtin University in Australia, and Evans, medical chief of the Montreal-based International Civil Aviation Organization, were on the emergency committee that advised WHO's Director-General Margaret Chan before she declared swine flu a pandemic.
WHO convened the panel in April to conduct a "credible and independent review" of how it and national authorities handled the outbreak. Concerns were raised at the time that several panel members were trusted WHO advisers and government employees who could end up whitewashing any failures.
The review panel will present a final report next year.
Harvey Fineberg is Dr. Harvey Fineberg, head of the Institute of Medicine in Washington, DC. He also is the former head of the Harvard school of public health, and former Harvard provost. But to flubies, Harvey is best-known as the co-author of the seminal study of the 1976 swine flu debacle, along with the late historian Richard Neustadt. Harvey is also a pen pal of mine, and I engage him occasionally as a sounding board for ideas that, depending on his thoughts, eventually appear here as blogs.
Harvey may be the most-qualified person in the world to assess the WHO's handling of the 2009-10 swine flu pandemic. His 1976 study should be required reading for anyone who is interested in public policy when it comes to public health and infectious disease policy. I am equally certain his committee's analysis of the WHO's conduct during this latest pandemic will also be compelling reading.